Kratom Part 1: What It Is, How It Works, Potency Differences, Traditional vs. U.S. Use, and Why Caution Is Essential
Introduction: Why Kratom Deserves a Careful, Research-Driven Look
Kratom (Mitragyna speciosa) has become one of the most talked-about herbal substances in the United States over the past few years. Marketed as a “natural” energy booster, pain reliever, mood enhancer, or “legal opioid alternative,” kratom has gained popularity among people searching for relief from fatigue, anxiety, alcohol substitute, or opioid withdrawal. Yet emerging scientific evidence, rising poison-control calls, growing concerns from the FDA and DEA, and dramatic differences in product potency reveal a much more complicated, and potentially dangerous, picture than most consumers realize.
In recent years a stronger version of Kratom, 7-Hydroxymitragynine (7-OH) has been introduced. This version is of grave concern for being highly addictive and causing withdrawal symptoms that often leave the individuals needing hospitalization and often in Intensive Care Units (ICU).
Kratom is not a new substance, even in the United States, but the presence of it over the past few years has greatly grown. Kratom has been used for hundreds if not thousands of years in Southeast Asia, and research on this plant have existed for years.

This Part 1 blog provides a comprehensive, research-based overview of:
What kratom is
How it affects the body
The key alkaloids (mitragynine and 7-hydroxymitragynine)
Traditional vs. modern usage patterns
How kratom products are manufactured today
Potency differences between Southeast Asia and U.S. markets
Foundational safety concerns
Frequently asked questions
Key takeaways for individuals and families
Part 2 (published separately) will examine legality, withdrawal symptoms, side effects, addiction patterns, and routes to treatment.
If possible, a Part 3 will be published on Recover Clarity’s blog section which will examine how such a dangerous substance continues to be allowed to be produced and distributed in the United States. This research will be difficult to uncover, but the concerns in the US have existed for almost a decade.
What Is Kratom? A Complete Overview
Kratom is a tropical evergreen tree native to Thailand, Malaysia, Indonesia, Papua New Guinea, and the Philippines. Classified within the Rubiaceae (coffee) family, kratom shares some botanical characteristics with coffee, but the similarities end there when it comes to pharmacology and effect. The effects of this plant are more aligned with that of opioids than they are with caffeine such as with coffee, however traditional uses were for energy in Asia.
Botanical Characteristics
Mature kratom trees can grow 40–50 feet tall with a large canopy spread.
Leaves are broad, glossy, and rich in alkaloids, which are chemical compounds responsible for their psychoactive effects.
The plant naturally produces over 40 alkaloids, with mitragynine making up most of the leaf’s active profile.
7-Hydroxymitragynine (7-OH) is another alkaloid in kratom tree, but only makes less than 2% of the total alkaloids (U.S. Food and Drug Administration, 2025b)
Historical Footprint and Early Documentation
No precise “first use” date exists, but kratom has a long history in Southeast Asian medical and cultural traditions. Scientific literature first referenced kratom in 1836, suggesting that locals had used it for decades or centuries before. Workers commonly chewed leaves or brewed teas for stamina and pain relief.
The author of this blog recently traveled through Southeast Asia and was in Thailand in late 2025. Talking with locals they expressed knowing of many generations which used the kratom leaves in previous years. Specifically, those in the northern regions of Thailand and in the Golden Triangle (historic for opium trade), discussed with me that generations have used this plant with little concern of addiction.
Kratom’s Arrival in the U.S.
Although kratom has deep roots in Southeast Asia, it did not achieve meaningful presence in the United States until the early 1990s. The U.S. Food and Drug Administration recorded the first known kratom dietary supplement marketing date as October 15, 1994 (U.S. Food and Drug Administration, 2025a).
One method of seeing growing concerns is the case mentions by the Poison Centers. From this data we can see a trend especially in recent years of the amount that Kratom is mentioned with drastic increases since 2020 (America’s Poison Centers, 2025; Anwar et al., 2016; Gummin et al., 2024).
The version of 7-OH is not directly mentioned and is stated to be included in the case mentions for Kratom. But the partial year data for 2025 shows an even larger spike in case mentions, which 7-OH could contribute to, but this is unknown at this time (America’s Poison Centers, 2025).
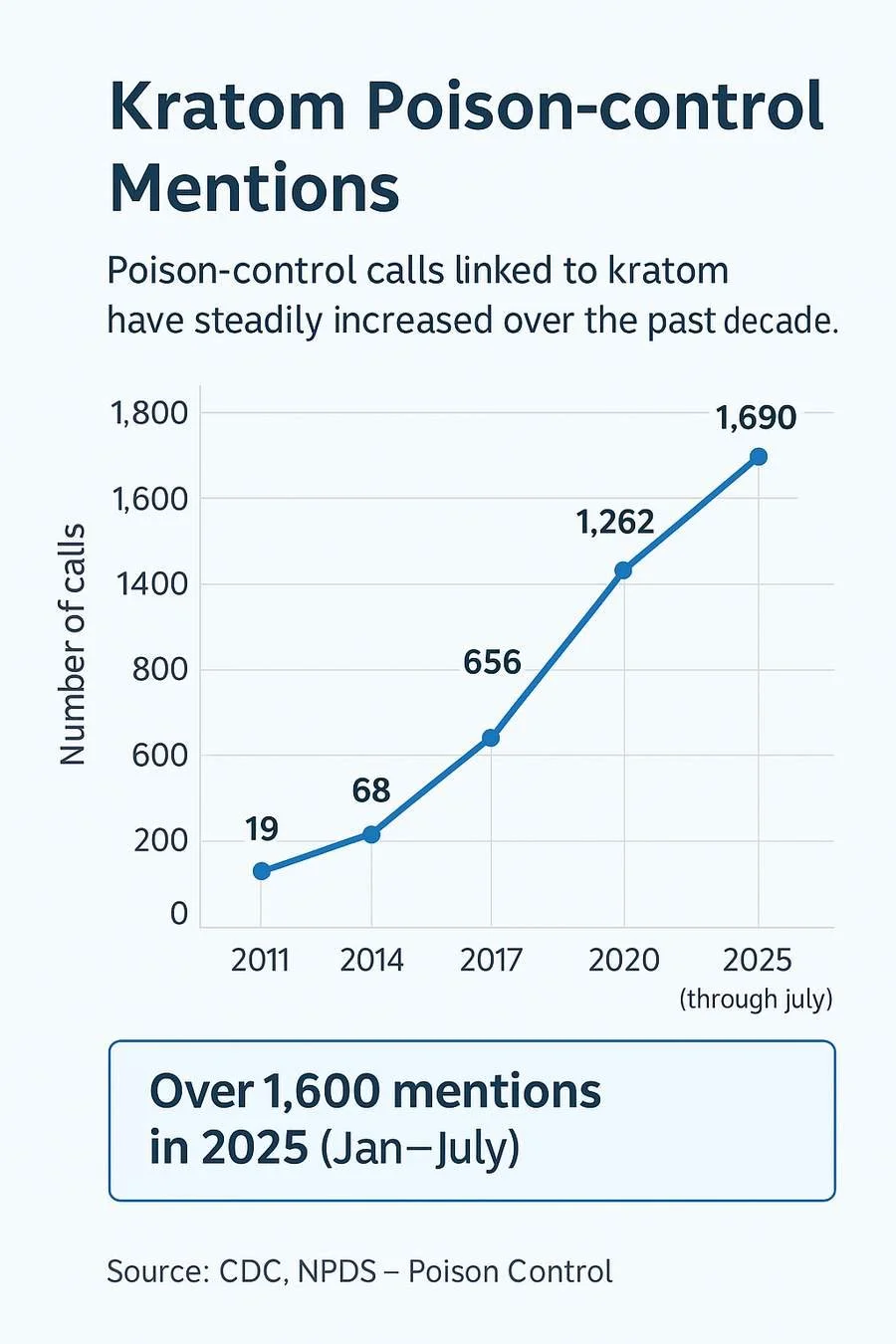
This chart illustrates the rise in kratom-related poison control mentions in the United States from 2011 through 2025. Data from the Centers for Disease Control and Prevention (CDC) and the National Poison Data System (NPDS) show a steady increase in reported exposures, with more than 1,600 mentions recorded in the first seven months of 2025. The trend highlights growing public health concerns, particularly as high-potency kratom extracts and 7-hydroxymitragynine products become more widely available.
Seeing comparisons of specific substance data can be difficult to find. Detailed poison-control exposure counts for cocaine, methamphetamine, and fentanyl in 2023 (or other years) are not currently available in publicly released National Poison Data System (NPDS) reports. NPDS annual reports often include overall case totals and “class” categories (e.g., analgesics, household products), but specific illicit drug totals are not typically published publicly by NPDS. The data that is available are for the substances of LSD and PCP for 2022, which is the most recent available data for these substances (Drug Enforcement Administration, 2023).
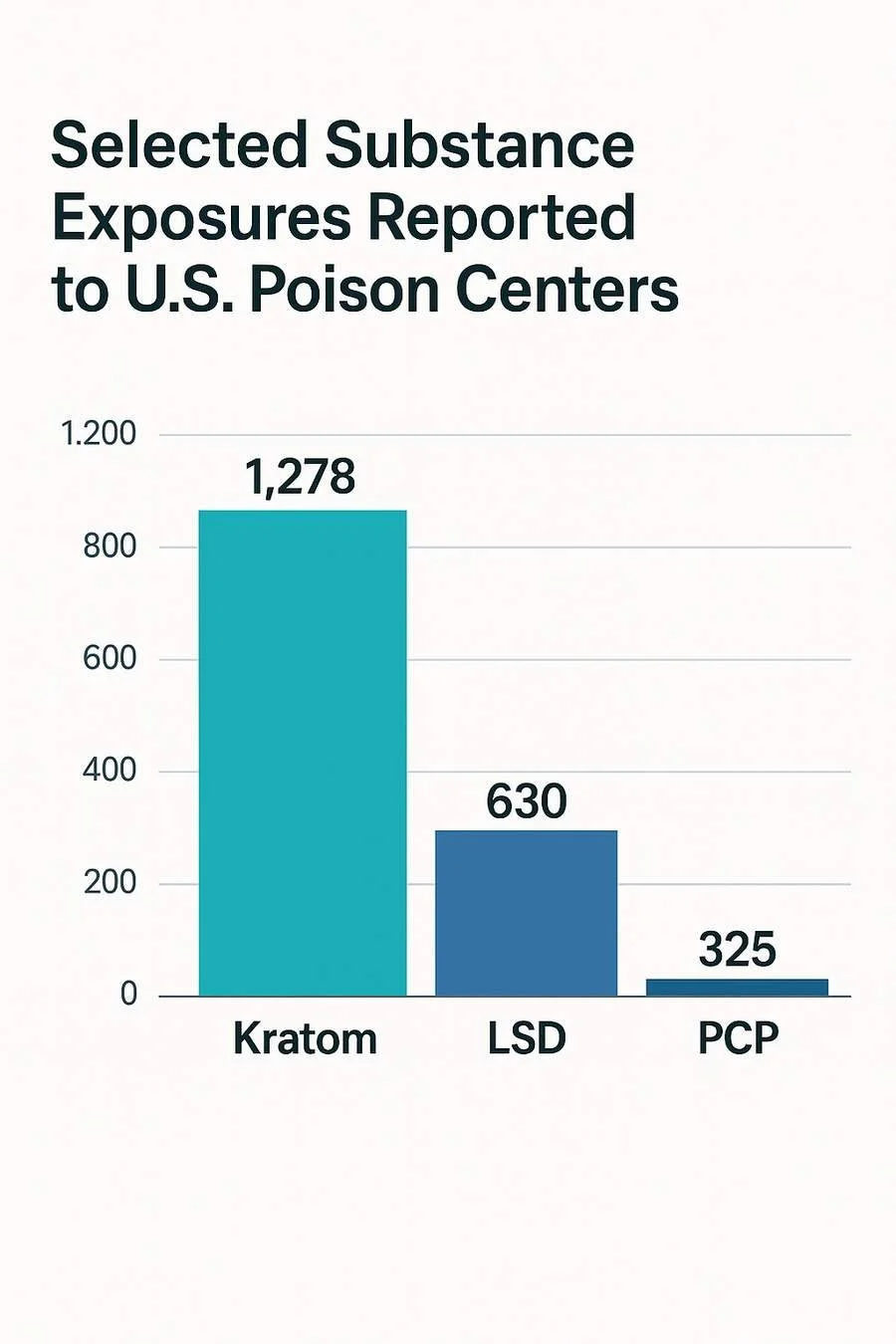
This chart compares selected substance exposures reported to U.S. poison centers, highlighting higher reported kratom-related exposures relative to LSD and PCP. Data are derived from the National Poison Data System and illustrate trends relevant to public health monitoring and substance use risk assessment.
While poison-control data does not equal prevalence, it strongly signals growing harm, confusion, and misuse.
How Kratom Affects the Body
Kratom’s pharmacology is complex and not yet fully understood. It interacts with the body very differently than caffeine, despite the botanical relationship to coffee. We are recently seeing how this substance is more like that of opioids because of the effects on the mu-opioid receptors, like that of opioids. This is even more true about the 7-OH extract of Kratom.
Key Alkaloids: Mitragynine and 7-Hydroxymitragynine
The two most important psychoactive alkaloids in Kratom are:
Mitragynine
The most abundant alkaloid in kratom leaves
Acts partially on mu-opioid receptors, leading to opioid-like effects
Can be converted by metabolism into 7-hydroxymitragynine
7-Hydroxymitragynine (7-OH)
Far more potent, even in small amounts
Has a significantly stronger affinity for mu-opioid receptors
Increasingly found in concentrated U.S. kratom products
Of major regulatory concern, leading the FDA in July 2025 to announce significant steps toward controlling 7-OH as a Schedule I substance (FDA, 2025b).
Other Alkaloids in Kratom
Lesser-known alkaloids also contribute to kratom’s complex effects:
Speciociliatine
Speciogynine
Paynantheine
While these alkaloids are not as psychoactive as mitragynine or 7-OH, their combined presence influences kratom’s physiological and psychological effects. More research is needed to fully understand the complexity of these alkaloids and how they affect the body and brain. Overall, there are up to 40 alkaloids in Kratom.
The Current State of Scientific Research
Preclinical Evidence, Limited Clinical Trials
Modern kratom research remains surprisingly limited, with most studies conducted in animals rather than humans. Scientists have explored:
How mitragynine converts into 7-OH
How kratom interacts with brain opioid receptors
Toxicity and organ-stress potential
Behavioral effects in animal models
However, clinical research on human subjects is lacking, meaning:
No standardized safety guidelines
No validated “therapeutic dose range”
No established long-term safety data
No verified medical benefits recognized by U.S. regulators
No FDA-Approved Medical Uses
The FDA has not approved kratom for any medical purpose.
The DEA lists kratom as a “Drug and Chemical of Concern.”
As of July 29, 2025, the FDA announced bold steps targeting the regulation of 7-hydroxymitragynine due to its potency and overdose potential (U.S. Food and Drug Administration, 2025b).
Without regulatory oversight, kratom products in the U.S. vary dramatically in potency, purity, and safety.
Traditional Uses vs. Modern Patterns of Use
Kratom’s reputation in Western markets is often shaped by marketing claims that contradict traditional practices. Kratom first appeared in scientific literature back in 1836, but it is expected that the use of this plant dates back centuries (Cinosi et al., 2015; Grovogui, & McCurdy, 2025).
Traditional Use in Southeast Asia
The traditional use of Kratom was by either chewing fresh leaves directly from the tree or brewing the leaves in tea. These delivery methods provide greatly lower doses of the alkaloids, in a fraction of what is more commonly seen in Western usage of Kratom.

As a Stimulant for Laborers
Workers traditionally chewed kratom leaves or brewed tea to:
Increase energy
Reduce fatigue
Alleviate muscle aches
In low doses, kratom acts more like a stimulant, which is consistent with its botanical relationship to the coffee plant.
As a Sedative or Pain-Relief Aid
In higher doses, kratom was historically used to:
Reduce pain
Promote relaxation
Act as a sedative
Manage opium or morphine dependence in early 20th-century Thailand and Malaya
Although some modern users in the U.S. claim that kratom helps withdrawal symptoms, self-medication often leads to switching one dependency for another. This is leading many individuals to seek treatment options similar to that for Opioid Use Disorder, such as the treatment provided here at Recovery Clarity with our Online Suboxone Doctors.
Recover Clarity treats kratom dependency as part of its addiction-treatment services in the Addictions We Treat.
Modern Use in the United States
Kratom usage patterns in the U.S. have change greatly from traditional usage of this substance. And this is where many of the current problems stem from. Many of the forms of Kratom and 7-OH are greatly concentrated well beyond that of the traditional usage of the substance.

Rising Use for Self-Treatment
Many individuals turn to kratom in attempts to:
Manage chronic pain
Reduce anxiety or depression
Self-treat opioid withdrawal symptoms
Enhance mood or productivity
The Problem of Dependency
The National Institute on Drug Abuse (2024) notes that overdoses from kratom alone appear rare; however, dependency is real. As kratom dependence increases, individuals may return to stronger opioids like heroin or fentanyl, which dramatically increase overdose risk.
How Kratom Is Processed and Consumed Today
Traditional Preparation Methods
Historically, kratom was consumed through:
Chewing fresh leaves
Brewing tea from dried leaves
Occasional smoking of dried leaves
A single kratom leaf typically weighs:
0.43 g to 1.7 g
Dependence-level users historically consumed kratom 3–10 times per day. Effects lasted approximately 1–1.5 hours.
Modern U.S. Kratom Products
Today’s U.S. market includes:
Powder-filled capsules
Bulk powdered leaf
Highly concentrated liquid extracts (“kratom shots”)
Gummies
Honey sticks
Resin extracts
Enhanced blends
The Problem of Zero Standardization
The FDA does not regulate kratom. As a result:
Alkaloid content is inconsistent
Product labels are often inaccurate
Some extracts contain far higher 7-OH levels than natural leaf
Products may include added adulterants
This lack of regulation is a core driver of modern kratom-related harm.
Why Potency Differences Matter - A Lot
One of the most important (and least understood) aspects of kratom safety is the massive difference in potency between:
Natural kratom leaf used traditionally
Extracted, concentrated kratom products sold in U.S. gas stations, vape shops, and online
Geographic Variations in Natural Potency
Kratom grown in different regions naturally varies in alkaloid content:
Thailand: up to 66% mitragynine
Malaysia: closer to 12% mitragynine
For consumers, this means not all kratom leaves are chemically comparable.
Typical Kratom Alkaloid Amounts in Southeast Asia
The European Monitoring Centre for Drugs and Drug Addiction (n.d.) reports:
Typical per-use mitragynine amount: ~22.5–25 mg
Typical daily maximum: ~75 mg (three doses)
These traditional amounts reflect mild to moderate physiological effects, not the high-intensity effects associated with modern extracts.
Concentrated U.S. Extracts: A Much Higher-Risk Category
Many U.S. kratom “shots” advertise:
250 mg mitragynine per 5 ml
Some exceed 375 mg per bottle
Labels often recommend:
“Do not consume more than 3 servings in 24 hours.”
Comparing Traditional to Modern Use
Traditional daily intake:
~75 mg mitragynine
Modern U.S. daily intake (3 extract servings):
250–375 mg × 3 = 750–1,125 mg
This is 10–15 times the traditional maximum exposure.
Even More Concerning: 7-Hydroxymitragynine (7-OH)
Some products are fortified with high concentrations of 7-OH, the more potent, more dangerous alkaloid.
These products more closely resemble semi-synthetic opioids than any naturally occurring plant.
Regulatory & Safety Considerations (Preview for Part 2)
Although Part 2 covers regulations in depth, a high-level overview helps contextualize why professional agencies are concerned.
No FDA-Approved Medical Uses
Kratom has zero FDA-recognized therapeutic benefits.
DEA Monitoring
Kratom is listed as a “Drug and Chemical of Concern” due to reports of dependency and harm. This is not a new concern, the DEA (2016) first mentioned the potential dangers of Kratom specifically with the alkaloids of mitragynine and 7-hydroxymitragynine (7-OH) in August of 2016. The DEA at this time wanted these to be placed under the Controlled Substance Act as Schedule I substances as this placement was necessary to avoid an “imminent hazard to public safety.” This was published in the Federal Register, but the DEA withdrew this intent in October of 2016 due to congressional objections and public backlash.
On January 22, 2025 the DEA has again placed Kratom (Mitragyna speciosa) as a “Drug and Chemical of Concern” on its official Drugs of Concern list (Drug Enforcement Administration, 2025a).
International Restrictions
Countries including Australia, Denmark, Finland, Malaysia, and Thailand (at various points) have restricted or banned kratom or its alkaloids. There are even certain parts of the United States that are banning Kratom. It is illegal in at least 16 countries, including some where the plant naturally grows.
Reported Adverse Outcomes
Dependency
Withdrawal symptoms
Organ toxicity
Dangerous interactions with other substances
Overdose fatalities
These concerns continue to grow and so does public health scrutiny.
Frequently Asked Questions About Kratom
Is Kratom the same as coffee?
No. They share a botanical family, but kratom interacts with the body through mu-opioid receptors, not caffeine receptors.
Is Kratom a stimulant or sedative?
It can act as both stimulant at low doses, sedative at higher doses, but effects vary widely due to inconsistent product potency.
Is Kratom approved for any medical purpose in the U.S.?
No. The FDA has not approved kratom for any medical use. 7-OH is being considered for Schedule I classification as of July 2025.
How long do Kratom’s effects last?
Typically 1–1.5 hours, depending on dose, product type, individual metabolism, and tolerance.
How do traditional preparations differ from modern U.S. products?
Traditional use involves chewing leaves or brewing tea, resulting in mild–moderate effects.
U.S. products include extracts, shots, potent powders, and enhanced blends, often with alkaloid levels hundreds of percent higher than natural leaf.
Key Takeaways
Kratom is under-researched: Scientific uncertainty means risks may be greater than known.
No FDA-approved uses: Kratom has no recognized medical benefits in U.S. regulatory frameworks. Meaning there are no regulations on Kratom manufacturing.
Risks are increasing: Dependency, withdrawal, contamination, and overdose cases are rising.
Potency varies dramatically: U.S. concentrates can exceed traditional potency by 10 to 15 times or even more.
Effects depend on dose and product type: Stimulant-like at low doses, sedative-like at high doses, but unpredictable due to lack of standardization.
If You or Someone You Know Needs Help
Kratom dependence is real, and many people struggle to stop using it, especially in the U.S., where products are far more potent than traditional preparations.
Recover Clarity offers evidence-based addiction treatment, including:
Kratom dependency treatment
Suboxone treatment for opioid use disorder
Telehealth access across Pennsylvania and West Virginia
Compassionate, confidential support
If you need help, please call us or complete our online inquiry for here Contact Us.
Coming Up in Part 2
In the next article, we’ll cover:
Kratom’s legal status in the U.S. & worldwide
Documented side effects and health risks
Withdrawal timeline and symptoms
Signs of kratom addiction
Treatment options and pathways to recovery
References
America’s Poison Centers. (2025, August 12). Health advisory: Serious illnesses associated with 7-OH use. America’s Poison Centers News & Alerts.
Anwar, M., Law, R., & Schier, J. (2016). Notes from the field: Kratom (Mitragyna speciosa) exposures reported to poison centers—United States, 2010–2015. Morbidity and Mortality Weekly Report, 65(29), 748–749. https://doi.org/10.15585/mmwr.mm6529a4
Cinosi, E., Martinotti, G., Simonato, P., Singh, D., Demetrovics, Z., Roman-Urrestarazu, A., … Corazza, O. (2015). Following “the roots” of Kratom (Mitragyna speciosa): The evolution of an enhancer from a traditional use to increase work and productivity in Southeast Asia to a recreational psychoactive drug in Western countries. BioMed Research International, 2015. https://doi.org/10.1155/2015/968786
Drug Enforcement Administration. (2023). LSD and PCP drug fact sheets.
Drug Enforcement Administration. (2025a, January 22). Kratom [Drugs of Concern]. U.S. Department of Justice. https://www.dea.gov/taxonomy/term/311
Drug Enforcement Administration. (2025b, October). Kratom (Mitragyna speciosa). Drug & Chemical Evaluation Section.
European Monitoring Centre for Drugs and Drug Addiction. (n.d.). Kratom (Mitragyna speciosa) drug profile. EMCDDA. Retrieved from https://www.emcdda.europa.eu/publications/drug-profiles/kratom_en
Grovogui, N., & McCurdy, C. R. (2025). Traditional use of kratom in Southeast Asia. In Ethnobotanicals and Functional Foods. UF/IFAS. https://edis.ifas.ufl.edu/publication/EP653
Gummin, D. D., Brent, J., Banner, W., et al. (2024). 2023 annual report of the National Poison Data System (NPDS) from America’s Poison Centers: 41st annual report. Clinical Toxicology, 62(12), 793–1027. https://doi.org/10.1080/15563650.2024.2345678
National Institute on Drug Abuse. (2024). Kratom. National Institutes of Health.
https://nida.nih.gov/research-topics/kratom
U.S. Food and Drug Administration. (2025a, July 29). FDA and kratom.
U.S. Food and Drug Administration. (2025b, July 29). 7-hydroxymitragynine (7-OH): An assessment of the scientific data and toxicological concerns around an emerging opioid threat [PDF]. https://www.fda.gov/files/drugs/published/7-hydroxymitragynin_7-oh_an_assessment_of_the_scientific_data_and_toxicological_concerns_around_an_emerging_opioid_threat.pdf